Surgery for a watery eye (Lacrimal surgery)
Please note, this page is printable by selecting the normal print options on your computer.
This leaflet explains the options of treatment for a watery eye or one that becomes constantly sticky due to blockage of the tear drainage system (lacrimal system).
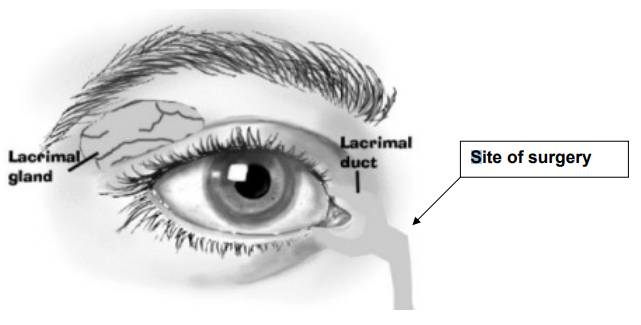
The tear drainage system of the eye starts with two small holes along the edges of the inner part of the upper and lower eyelids. It then continues into a sac along the side of the nose and finally opens up further down towards the back of the nose. Blockage can occur anywhere along this system. In some cases, there may not be an actual blockage of the tear duct but the eye waters because the normal pumping action of the duct is not very effective (functional block).
What can be done to help this?
Your symptoms may only be improved by an operation.
Is an operation my only choice?
If you do not have an operation, the symptoms of watery eye tend to persist but there is no danger to your eye or vision.
If I decide to have an operation will I need to stay in hospital?
Most patients are able to go home the same evening after surgery . Occasionally, patients may have to stay in overnight.
Is an anaesthetic required?
A general anaesthetic is usually required. In exceptional cases (e.g. when the risk of a general anaesthetic is deemed too high), the operation can be done under local anaesthetic.
What happens during the operation or procedure?
There are two main approaches to lacrimal surgery. These are external (external dacryocystostomy) or via the nose (endonasal dacryocystostomy). The technique which is performed via the nose may be surgical or with a laser. There may be slight variations in the procedure and success rates depending on the position of the tear duct blockage. Both external and endonasal DCR surgery involves opening up the tear sac and adjacent bone so that there is a direct connection between the sac and the inside of the nose (upper end) bypassing the blockage in the tear drainage system.
External DCR involves making a cut in the skin along the side of the nose whilst endonasal DCR (the procedure through the nose) does not require this and involves the expertise of an Ear, Nose and Throat Surgeon and an Eye Surgeon. Silicone tubes are usually inserted through the surgical opening to stop it from closing. One end of the loop will be visible in the corner of the eye whilst the other end will be inside the nose. This tubing is usually removed 3 months after surgery.
* Removal of this tubing is a simple procedure and is done in the outpatient clinic with only mild discomfort felt.
What are the risks and benefits of these operations/procedures?
External DCR
The success rates for this surgery vary from 50 to 96% depending on where the blockage is. The success rate improves when the obstruction is closer to the nose and gets less when it is present nearer the eyelid or is a functional block. With functional blocks there is a 25% chance of making the watering worse.
Possible post-operative complications include:-
• infection (8%)
• wound scarring or numbness (20%)
• bleeding
These complications are rarely serious but do require management. Infection and bleeding can usually be treated effectively. Skin numbness also tends to improve with time. Very rarely, one can get more serious problems like double vision or loss of vision.
Endonasal DCR
Success rates for this approach range from 54% to 93% depending on the level of obstruction as for external DCR rates and also whether the blockage is functional. Possible complications from surgery include bleeding and air being trapped under the skin (orbital emphysema). Again these are not very serious and can settle spontaneously or be treated. Double vision and loss of vision can very rarely occur.
Congenital lacrimal obstruction
Blockage of the tear drainage system can occur in children because it has not developed normally from birth (congenital blockage). This type of blockage usually has a very good outcome as 96% of cases resolve naturally by the age of 12 months. Of those that do not resolve, the drainage system can be examined and possibly unblocked by passing a narrow instrument into the duct. This is done under general anaesthetic and there is no cutting of skin. Success rates for probing correlates inversely with increasing age:
| Age | Success Rate Percentage |
| 12 months | 92% |
| 24 months | 89% |
| 36 months | 80% |
| 48 months | 71% |
| 60 months | 42% |
Possible complications include bleeding (20%), local trauma to the drainage system resulting in scarring, and the creation of additional false passages, all of which may make the watering worse. These problems can usually be rectified but may require additional procedures.
How will I feel after the operation?
You will be given pain relief whilst in hospital and on discharge will be given a prescription for pain relief to be taken at home if required.
Follow-up
When you are discharged you will be given an appointment to attend as an outpatient 2 weeks after your operation. Following this appointment, you will be reviewed at 3 months and again at 6 months.
Useful contact numbers
Ophthalmology Outpatients Reception 01908 660033 Ext 2829
References can be supplied for the information contained within this information leaflet if required.