Endoscopic Retrograde Cholangiopancreatography (ERCP)
Please note, this page is printable by selecting the normal print options on your computer.
You have been advised by your consultant to have an investigation known as an ERCP.
This procedure requires your formal consent. This booklet has been written to enable you to make an informed decision in relation to agreeing to the investigation. You will be required to sign a consent form on the day of the procedure, which is a legal document, therefore please read this booklet carefully beforehand.
If you are unable to keep your appointment, please notify the endoscopy unit as soon as possible. This will enable staff to give your appointment to someone else and to re-arrange another date and time for you.
You need to understand all the information, including the possibility of complications. There will be the opportunity to speak to a health care professional about anything that you do not understand on the day of the procedure before you sign the consent form.
What is an Endoscopic Retrograde Cholangiopancreatography (ERCP)?
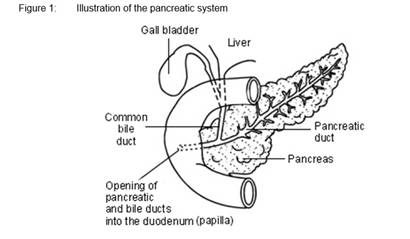
This is a test which allows a doctor to look at the tube draining the liver and gallbladder (also known as common bile duct) and the tube draining the pancreas (also known as main pancreatic duct). The doctor will pass a thin tube through your mouth, down through your stomach and then into the first part of the intestine (duodenum). Then some dye will be injected into the common bile duct and the pancreatic duct through a little opening called the Papilla. X-rays will be taken at this time.
Are there any alternatives to an ERCP?
Scans, such as an ultrasound, MRI or CT scan, can show problems with the bile duct or pancreatic duct and help give an accurate diagnosis. However, treatments of the ducts cannot be given during these tests. This requires an ERCP. ERCP is therefore recommended when treatment or intervention is needed. Other alternatives to access the bile duct, include procedures through the skin under x-ray guidance or surgery. However, ERCP is frequently the best option for treating these conditions.
How do I prepare?
Because the test involves x-rays, it is important that, if you are female and of a childbearing age, you inform us when your period is due so that the procedure can be done within the first ten days from the first day of your period. If you have been sterilised or have had a hysterectomy, please let us know.
Do not have anything to eat or drink for at least 6 hours (preferably overnight) before the procedure.
What about my medication?
- Routine Medication: If you are on any medication, especially blood pressure tablets, you should take these with a sip of water as usual.
- Diabetes: If you are diabetic, it is important that you contact your diabetic specialist nurse or assessment nurse prior to any of these preparations so that they can instruct you on what you need to do.
- Anticoagulants/ Antiplatelets: If you are taking blood-thinning medicines, such as Warfarin, Dabigatran, Heparin, Dalteparin, Apixaban, Clopidogrel, the dose of these may need to be altered or stopped before your procedure. You may also need to have blood tests before your procedure. If the referring doctor did not give you instructions, you may be referred to the bridging clinic for advice on stopping your medication. If this is required, this will be arranged for you by the referring clinician or the endoscopy booking coordinator.
What to bring with you?
Along with your appointment letter you will have received a health questionnaire. Please complete it and bring it with you. You will also find enclosed a copy of your consent form; please read this carefully but do not sign it. This is just an example for you to read carefully prior to your appointment. The endoscopist will meet with you prior to your endoscopy to discuss what is going to happen, any risks and any serious or common side effects. At this point you will be given the opportunity to ask any questions and then you will sign the ‘actual’ consent form. You will also need to bring a dressing gown and a pair of slippers.
After your procedure you will be offered a choice of hot drink and biscuits. If you have any allergies/ intolerance, you might want to bring a snack as we are unable to cater for all dietary requirements.
How long will I be in the Endoscopy unit?
You should expect to be in the unit for approximately 6-8 hours. Please note that the time of your appointment is not the time that the procedure will be performed.
How long you will be in the unit will depend on how quickly you recover from the procedure, the sedation you may have had and on how busy the unit is. The unit also looks after emergencies, and these can sometimes take priority over outpatient procedures. You should be kept informed of any delays but if you have any questions or concerns, please ask a member of the staff.
What happens when I arrive?
After checking in at reception, a qualified nurse will welcome you and take you to the admissions area where you will have a brief medical assessment. Please note that the endoscopy unit operates a same sex environment and your relative may not be able to accompany you past the waiting area unless there are exceptional circumstances.
In the admission room, you will be asked some questions regarding your medical and surgical history to confirm that you are fit to undergo the procedure and about your arrangements for getting home. The nurse will make sure that you understand the procedure and discuss any questions you may have.
Your blood pressure, heart rate, respiration and oxygen levels will be recorded. If you have diabetes, your blood sugar level will also be checked and recorded. In preparation for sedation, which will be given later, the nurse will insert a cannula (a small plastic tube) into a vein in your hand or arm.
You will be asked to put on a hospital gown. If you wear spectacles or dentures, you will be asked to remove them. All your belongings will be kept with you throughout your procedure to prevent anything being lost. It is advisable to leave any valuables at home as we do not accept responsibility for them.
Sedation
You will be given an intravenous sedative (usually Midazolam) and a painkiller (usually Pethidine or Fentanyl) which will be administered through an IV cannula (a plastic tube) which is inserted in a vein in your arm/hand. This will make you lightly drowsy and relaxed, but not make you go to sleep like a general anaesthetic. You will still hear what is said to you and therefore, will be able to carry out simple instructions during the procedure. Some people do not remember anything about the procedure once the effects have worn off.
Whilst you are sedated, we will monitor your breathing, respiration, and pulse rate via a finger probe, so that any changes can be recorded and dealt with accordingly. You will also be given some oxygen via a nasal sponge into your nostril. Your blood pressure may also be checked and recorded.
As you are having sedation, you must arrange for a responsible adult to collect you and stay with you overnight. If you have not been able to make these arrangements, you will not be able to have the procedure. You should not drive, return to work, operate machinery, or drink alcohol for 24 hours after the procedure, nor should you make any important decisions. The reason for this is that the sedation may, even though you may feel perfectly normal, still be in the body and may impair your judgement.
The ERCP procedure
After signing your consent form in the admission area, you will be escorted to the procedure room, you will be introduced to the team and a verbal safety checklist (called “WHO”) will be done. Your throat will be made numb by using the local anaesthetic spray; you will then be asked to lie in prone position (on your tummy) with your arms by your side. A mouth guard is placed lightly between your teeth.
Once an x-ray of your bile duct is taken the sphincterotomy (small cut inside) can be performed by the endoscopist, sometimes to gain access to the bile duct and this will enable him to remove the gallstones. You will not feel the cut being done. If a narrowing is noted in the common bile duct, the doctor may bypass the narrowing using a tiny tube called a stent which is placed at the same time the ERCP is performed. This will enable the bile to drain freely. Sometimes some small biopsies (tissue samples) are taken to look at under the microscope.
The procedure usually will take between 30 and 60 minutes. Occasionally the procedure can be longer.
Milton Keynes University Hospital is a teaching hospital and there may be a student and/or a trainee present in the room or a supervised trainee may be doing your procedure. If you have any concerns or objections, please contact the Endoscopy Unit prior to your test or make the nurse admitting you aware of this.
Aftercare
After the procedure, you will remain in the Endoscopy Unit for about 4-6 hours. You may have some abdominal bloating due to the air which has been pumped into your stomach during the procedure. You may be given a suppository for pain relief. A Diclofenac suppository may be administered to help reduce the infection. The nurses will advise you when you can eat and drink.
When do I know the result?
Usually, the doctor or nurse will be able to tell you the results straight after the test, or if you have been sedated, when you are discharged. However, if a sample (biopsy) has been taken for examination, the results may take several weeks. Details of results and any necessary treatment should be discussed with your consultant. A nurse will discharge you, discuss any aftercare and follow up needed and answer any questions you may have. Before leaving you should receive written information on your procedure and a copy of the consent form.
Being collected after the procedure
If you are having sedation, the person collecting you must come to the unit to collect you. We advise that they park in the multi-storey car park before reporting to the Unit.
Are there any risks?
ERCP does have some risks associated with it. The doctor will explain them to you before you sign the consent form. These are not common complications, but it is important that you are aware of them. Some of these may be related to the medication given (sedative).
The possible complications of ERCP are listed below. Any numbers which relate to risk are from studies of patients who have had this procedure. Your doctor will tell you if the risk of complications is higher or lower for you.
- Sore throat, which gets better quickly.
- Allergic reaction to equipment, materials, or sedative. The endoscopy team is trained to detect and treat any reaction that may happen. Let the admitting nurse and endoscopist know if you have any allergies or you have reacted to any drugs or tests in the past.
- Breathing difficulties or heart irregularities, as a result of reaction to sedation or inhaling secretions such as saliva. To help prevent this from happening, your respiration and oxygen levels will be monitored, and a suction device will be used to clear any secretions. Rarely, a heart attack or stroke (loss of brain function resulting from an interruption of the blood supply to the brain) can happen if you have serious medical problems.
- Aspirating fluid in airway (minor risk)
- The risk of Perforation (tear of the small bowel or bile duct) and Bleeding occurring is less than 1 in 100 examinations If a hole occurs, you will need to be admitted to hospital for further treatment which may include surgery.
- Damage to teeth and bridgework. The nurse will place a plastic mouthpiece in your mouth to help protect your teeth. Let the endoscopist and nurse know if you have any loose teeth or dentures.
- Incomplete procedure. This can happen due to a technical difficulty, food or blockage in the upper digestive system, complications during the procedure, or discomfort.
- Sedation. This can occasionally cause problems with breathing, heart rate and blood pressure. If these problems do occur, they are usually short lived. Careful monitoring by the endoscopy team ensures that any potential problems can be identified and treated quickly. Older patients and those with significant health problems, such as breathing difficulties due to a bad chest, may be assessed by a doctor or specialist nurse before having the procedure.
- Other risks may be due to the ERCP procedure itself like Pancreatitis (inflammation of the pancreas). The risk of pancreatitis varies between 5-10%. Cholangitis (an allergic reaction or an infection of the bile duct system) can be caused by the injection of the dye into the common bile duct.
- Bleeding, perforation – rare
- Risk of death – very rare.
Some of these complications may require a long admission to hospital, further scans, or treatments. Rarely, an open operation and prolonged admission to the Intensive Care Unit (ICU) may be necessary to manage a life-threatening complication. Very rarely, such complications can result in death. Risks vary, depending on why the test is being done, what is found during the procedure, what treatment is undertaken and whether you have other health problems. Sometimes the doctor may be unable to complete the procedure due to previous surgery on the stomach, or the effects of certain diseases on the upper bowel. You will have the opportunity to discuss the benefits, risks, and alternatives to ERCP with a doctor and a nurse before the procedure.
What to do if you feel unwell
After the procedure, if you feel ill, if you have any severe pain, fainting or if you notice any blood in your faeces or have any black stools, you must then seek urgent advice from the Endoscopy Department between 09:00 and 17:30 (01908 996 460) Monday to Saturday.
Outside these hours, please call a nurse on Ward 22 (01908 996 455) for advice or go to your nearest A&E department.