ACL Rehabilitation
Please note, this page is printable by selecting the normal print options on your computer.
What is the ACL?
The cruciate ligaments are a pair of extremely strong, thick ligaments in the centre of the knee joint. You have an anterior cruciate ligament (ACL) and a posterior cruciate ligament (PCL), they form a cross, this is where the name cruciate is derived. The ACL lies in front of the PCL running from the outer aspect of the femur (thigh) to the inner aspect of the tibia (shin).

Functions of the ACL
- To prevent forward movement of the tibia on the femur.
- To link the rotation of the upper leg to the lower leg when twisting and turning.
- The fine feedback sensors in the ACL provide information to the muscles which prevents excessive movement. If there is excessive movement, this can increase the possibility of cartilage tears.
How does an injury to the ACL occur?
An ACL injury can result in a complete tear of the ligament (rupture), where all the fibres are torn; or a partial tear where only some of the fibres are torn.
- Predominantly twisting injuries.
- Sports that involve deceleration, twisting cutting or jumping.

Treatment
There are two options; conservative therapy and surgery. This is a discussion you will have with your consultant. The outcome will be dependant on the demands of your everyday life.
In a non-athlete, or someone who does not need to do a lot of twisting and turning activities it is possible to rehabilitate to the previous level of function without surgery (conservatively).
The improvement of muscular control around the hips and knees will allow you to compensate for the loss of the ligament. Many runners are able to function by the bias of the hamstring muscles to inhibit the forward movement of the femur on the tibia.
Surgery
ACL reconstruction is the most common type of ligament reconstruction performed around the knee. Surgery is carried out to replace the stabilising function of the anterior cruciate ligament.
What does it involve?
The remains of the damaged ACL are removed and it is replaced with another form of soft tissue, called a graft.
A number of different types of grafts can be used to replace the ACL:
- Use of the hamstring tendons (semitendinosus and gracilis)
- Bone tendon bone (BTB) or patella tendon graft.
The preference of the Milton Keynes Surgeons is to use hamstring grafts as first choice. The evidence in the medical literature is that there is little or nothing to choose between these two main grafts in terms of results.
ACL reconstruction is usually performed using arthroscopic (keyhole) surgery. There is however a small (4-5 cm) incision below the knee where the tendons for the graft are taken from. ACL reconstructions may be performed either as day case or overnight surgery.
In patients who comply with rehabilitation (9-12 months), there is a 90 to 95% chance of a good result, whereby enough stability is restored to allow the patient to undertake activities, including sports that they were previously unable to do.
Following surgery you will be advised that you are to remain partial weight bearing on your operated leg for two weeks. This means that you can only put 50% of your body weight through the operated leg with the aid of two elbow crutches.
You will be advised by your physiotherapist when to stop using your crutches at your outpatient appointments. Your rehabilitation will take a minimum of 6-9 months to complete if you wish to return to full function, specifically sports.
If you fully comply with the rehabilitation program as advised you will be able to post surgery:
- Jog at 14 weeks
- Return to active sports 8-9 months
- Return to contact sports 9-12 months
- Possible complications of surgery include:-
- Infection, swelling, stiffness, discomfort and the new graft can re-rupture.
- Approximately 10-15% of all surgical patients may require a second smaller operation during rehabilitation for stiffness and/or cartilage injury.
NB – Do not perform any of the exercises unless advised to by your physiotherapist
Early stage exercises
Knee Flexion/Extension

This exercise is to increase range of motion of the knee and assist in the reduction of pain and swelling.
In sitting or lying keep your foot in contact with the floor and slide your heel towards your bottom hold for 5-10 secs. Then straighten your knee pushing it into the floor hold for 5-10 secs. Repeat x10-15.
Static Quadriceps Contraction
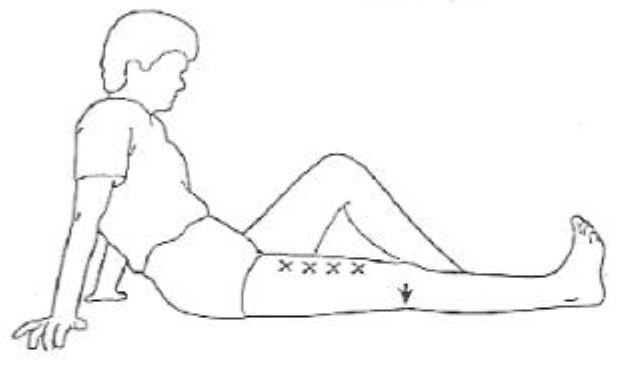
This exercise is to increase range of motion of the knee and increase muscle strength.
In sitting or lying keep your foot in contact with the floor straighten your knee pushing it into the floor hold for 5-10 secs. Repeat x10-15.
Bridging

The exercise strengthens your Gluteals (bottom muscles).
Crook lying position, neutral pelvis. With this exercise, imagine that your spine is a “necklace of pearls” à each vertebra being the pearl. Lift you tailbone towards the ceiling and continue to lift your spine off the mat (“one pearl at a time”), until you are resting on your shoulder blades. Hold the position for 10 secs, then slowly lower one bone at a time until your tailbone touches the mat. Repeat for 10 times.
Clam Level 1

You should feel this working your hip muscles.
Lying on your side with the spine in neutral, hips bent to 45º and knees bent up to approx. 90º. Lift the top knee upwards, keeping your feet together hold 5 secs. Then lower the top knee onto the bottom leg. *Do not let your pelvis roll backwards. Repeat 10 times on each side.
Hamstring curls in prone with hip extension

This exercise strengthens your hamstrings and gluteals.
Lying on the floor on your front, lift your foot up towards your bottom until the foot is facing the ceiling. Then squeeze your bottom and lift your knee 1-2 inches away from the floor, pushing your foot towards the ceiling. Hold for 5 secs. *No movement should come from your lower back, if there is movement, the exercise is too difficult, and you should keep your knee on the floor. Repeat 10 times.
Small knee bends
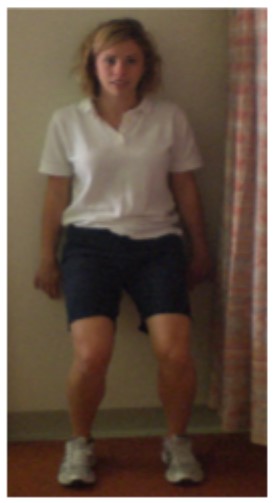
This exercise will strengthen your quadriceps (front of thigh) and improve your control.
Standing with your feet hip width apart and facing forwards. Keeping your back straight, flex the knees, keeping your weight in your heels, not allowing your knees to come forwards over your toes. Hold for 10 secs. Repeat 10 times.
The difference between good and bad pain
After major knee surgery your knee will be sore. It is important to understand that discomfort is normal particularly when performing some of the stretching exercises. In addition, your knee may ache after an exercise session. This is expected and normal so long as it is not associated with any significant increase in swelling. ‘Bad pain’ is usually sharp and severe in nature. It may be brought on by pushing too hard and it may be accompanied by an increase in swelling. Activities causing such a problem should be stopped and advice sought from your physiotherapist.