Abdominal Perineal Resection of the Rectum
Please note, this page is printable by selecting the normal print options on your computer.
Introduction
Abdominal Perineal Resection of the Rectum is the name given to the operation to remove the diseased part of your bowel. The operation can be done in two ways:
- It can either be performed in the traditional method of opening up the tummy from above your navel (tummy button) down in a straight line (approximately twenty centimetres in length). This is called ‘open’ surgery. The back passage is also removed and permanently stitched up. The wounds (the one on your tummy and the one on your bottom) will either be stitched, stapled or glued back together at the end of the operation and will heal in ten to fourteen days in an uncomplicated case.
- Or the operation can be performed laparoscopically. The other names for laparoscopic surgery are ‘keyhole’ surgery, minimal access surgery or minimally invasive surgery. A laparoscope is like a thin telescope with a light source.
The laparoscope is passed into the abdomen through a small incision (cut) in the skin often referred to as a port. It is used to light up and magnify the structures inside the abdomen. This is then connected to a television monitor so that the surgeon can see clearly inside the abdomen. Fine instruments are then passed into the abdomen through three or four small incisions in the skin. These instruments are used to lift, cut and take a small sample of tissue (biopsy) from inside the abdomen. The decision of which method is used to perform your operation will always be made with your best interests in mind and discussed with you. However, occasionally it is necessary to abandon laparoscopic surgery and open up the abdomen, if it becomes difficult to proceed safely with laparoscopic surgery.
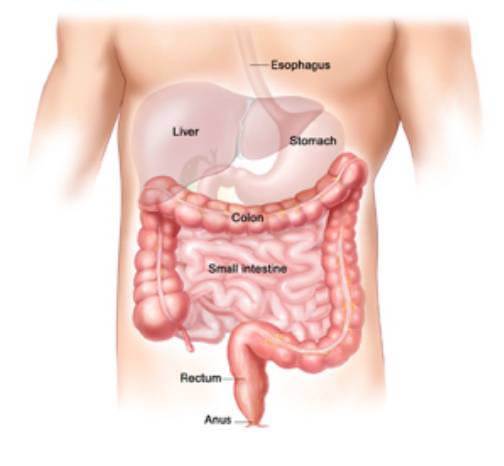
The Large Bowel
The large bowel (intestine or colon) is approximately 1.5 metres long. This part of the digestive tract carries the waste from digested food from the small bowel and gets rid of it as waste through the opening in the back passage (anus). Cells that line the bowel may begin to grow abnormally, forming a tumour (a growth of cancer cells). Tumours start in the lining of the bowel and can grow through some or all of the other layers.
Treatment Options
Bowel cancer can be treated in a number of ways, with people often having a combination of treatments. Your treatment will be designed to your individual needs and may include:
- Surgery, which this leaflet explains.
- Radiotherapy is used for some people as the initial treatment for cancer in the rectum (back passage). This is to shrink the tumour and make it easier to remove with an operation.
- Chemotherapy (use of drugs to treat the tumour) is sometimes used either before or after surgical removal of the cancer.
Abdominal Perineal Resection of the Rectum
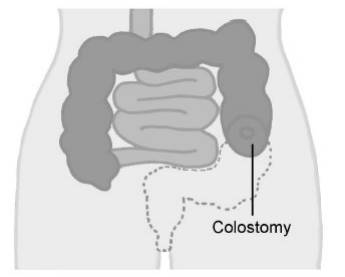
Removal of the diseased part of the bowel by an operation is the best treatment for a tumour of the bowel. The aim is to give you the best chance of a cure through total removal of the tumour. This operation is usually done to remove a tumour in the lowest part of the rectum (back passage). The rectum (back passage) and the opening into the back passage are removed and the area is stitched up closing your bottom completely. The end of the large bowel is brought out through the tummy as a permanent colostomy (stoma) and allows the bowel to empty into a stoma bag. You will see the stoma nurse specialist before your surgery for help and advice and she will also give you written information about a colostomy.
Please feel free to contact the stoma nurse on 01908 996 951 and ask for ext. 3070.
In women depending on where the tumour is it is sometimes necessary to remove part of the vagina if it is involved with the tumour. This can result in a much smaller vagina which may make sexual intercourse difficult or impossible.
Diagram of an Abdominal Perineal resection of rectum:
Risks of this operation
Any operation carries a risk, the risks of ALL operations include:
- Chest Infection. This would require antibiotics and physiotherapy
- Blood Clots in the legs (deep vein thrombosis) or in the lung (pulmonary embolism). We decrease this risk by using elastic stockings and blood thinning injections.
- Anaesthetic. The operation will be carried out under a general anaesthetic (you will be asleep). If you would like an explanation sheet about general anaesthetics and the associated risks please ask for one. If you are at increased risk because of other medical problems you may have your consultant will refer you to an anaesthetist for a formal assessment.
- Bleeding. This can occur with any operation
- Patients who are very overweight, smoke or have other medical problems are at increased risk of all of these complications
- Compartment Syndrome – Compartment syndrome is a rare but painful and potentially serious condition caused by bleeding or swelling to an enclosed space within the muscles. The pressure within the space can increase to such an extent that it affects the function of the muscle and nerves. The area most likely affected with the operation you are having is the legs, this is due to the position your legs have to be in during the operation, however it can affect your arms, tummy or the cheeks of your bottom. Pain is the most common symptom followed by numbness.
The treatment is an operation called a fasciotomy. The surgeon would need to open the skin and muscle of the area affected to relieve the pressure and prevent permanent damage. The wound is
dressed but is not closed with stitches until approximately 48-72 hours later. You may not be allowed to get out of bed and weight bare until the wound has been closed.
The risks of this operation also include:
- Wound breakdown. The wound on your bottom is at risk from opening up and taking a long time to heal. This can be due to any radiotherapy treatment you may have had which can delay healing. It can also be due to the pressure applied to the bottom whilst sitting which reduces the blood supply. This is one of the reasons why we will get you out of bed as soon as possible after the operation.
- Pelvic Nerve Damage. There is a specific risk of damage to the nerves of the pelvis which supply control to the bladder and sexual organs. In a man this can lead to impotence (failure to have or maintain an erection or ejaculate). In a woman it can cause painful intercourse. In both men and women the bladder can be affected making it difficult to pass urine.
- Increased risk of infection. This is because the bowel is an organ that is full of bacteria. Infection of the wound can occur. Sometimes an infection may develop inside the abdomen in the form of an abscess. Antibiotics are given to help control the infection and sometimes drainage of an abscess is necessary.
- Bowel stops working. This is temporary but can cause bloating of the tummy and sickness.
- Damage to other internal organs whilst removing the tumour in particular the bladder and small tubes to the bladder from the kidneys.
- Colostomy. There are some risks with having a colostomy. The stoma nurse will discuss all of these with you before your surgery. This is a major operation that has serious risks of which a small number of people do not survive. Your consultant will discuss your individual risks with you and answer any questions you have. Measures are taken to reduce these risks; however it is not possible to stop all risks completely.
Risks of not having the surgery
Just as there are risks of having surgery there are also risks of not having surgery. These include:
- Symptoms such as pain and bleeding may become worse.
- The bowel could become completely blocked or even burst, which could lead to further complications and may need surgery.
- The cancer could also spread to other parts of your body. If you have been told you are to follow the enhanced recovery programme please read the enhanced recovery information sheet as some information will be different. Enhanced recovery is a way of preparing you for surgery so that your stay in hospital is as short as possible.
After Surgery
The recovery period after bowel surgery varies. It usually involves a stay in hospital from three to ten days (in uncomplicated cases) depending on whether you have had open or laparoscopic surgery. Immediately after your operation the following tubes may be in place to help us care for you:
- Pain control will be administered through either an epidural (tube into your back) or a drip (tube into the veins on your arm). This will help you move around more freely. As you recover, these will be removed and pain killers will be given in the form of tablets. The pain gradually eases, particularly once you are up and moving around.
- Fluids in the form of a drip in your arm will keep you hydrated until you are able to drink freely.
- A catheter (tube to your bladder) will drain your urine into a collection bag so we can accurately measure the amount.
- A drain into your tummy-this is a tube to drain fluid away from the operation site. This will be removed when it finishes draining which is usually within two to five days. These tubes will be removed as soon as possible depending on your recovery. The nursing staff will help you get you out of bed as soon as possible after the operation to reduce the risk of complications from the
operation.
Diet
You may be able to eat during the first few days of recovery but your appetite will probably be reduced. It is important to eat small frequent amounts of easily digested food. In the first few days, you will be given specific advice on what you can eat. Meals can be supplemented with nourishing soups and snacks and high energy drinks. The body requires lots of calories during the healing process. After the first few days, there is no special diet and we encourage you to build up to your normal diet as soon as you can tolerate it.
Bowel actions
The bowel may take a little while to recover and you may still experience the sensation that you need to go to the toilet in the usual way, these are just phantom feelings. Passing wind through the stoma is a sign that your bowel is starting to work again. It is normal for the bowel to be irregular and sometimes is necessary to give medications to either slow the bowel down or give mild laxatives to encourage the bowel to move. You may have no sensation that the colostomy is going to work, this is quite normal.
Exercise
You will be encouraged to get out of bed the following day and you will be seen by a physiotherapist who will help you to do this. You will be wearing elastic stockings to reduce your risk of a blood clot but moving around will also help. The physiotherapist will also give you deep breathing exercises for your lungs as this will help prevent chest infections. Lifting after abdominal surgery is not recommended for approximately six weeks after your operation. The stoma nurse will give you detailed advice on lifting.
Stoma Care
The stoma nurse specialist will see you regularly to give you help and advice on managing your stoma and you will be given all the equipment you need to do this. You have to be able to manage your stoma with out help before you can be discharged home. The stoma nurse will also visit you at home within a few days after discharge to monitor your progress.
Driving
Check with your insurance company about any exclusion they may have. This includes being under the influence of some pain medication. You must be able to perform an emergency stop and you are not excluded from wearing a seat belt.
When you go home:
When you go home you may find that on some days you feel better than on other days. It is quite normal to have ‘good’ and ‘not so good’ days. However it is important to contact the GP if any of the following occur:
- Discharge or leakage from the wound or drain site
- High temperature
- Uncontrolled shivering/feeling hot then cold
- Pain when passing urine/frequent need to pass urine or very offensive smelling urine
- Difficulty with breathing, chestiness or cough with green or yellow phlegm
- Pain in the calf, leg or chest
- Abdominal pain which is different from the usual post operative soreness
- Bleeding from the back passage
- Vomiting
Results of your Operation
The piece of bowel that is removed is sent to the laboratory for detailed testing. The results will take ten to twenty days to be processed and a report will be sent to your consultant. These results will be used to determine if you need any further treatment. Your consultant or nurse specialist will then arrange an appointment with you to discuss the results.
Confidentiality
As part of your treatment some kind of photographic record may be made. For example, photographs or video. You will always be told if this is going to happen. The photograph or video will be kept with your notes and will be held in confidence as part of your medical record. This means that it will only be seen by those involved in providing care for you or by those needing to check the quality of care you have received. The use of photographs and video is also extremely important for other NHS work, such as teaching or medical research.
If we would like to use the information for these purposes we would only do so with your permission. We do not use any information in a way that identifies you.
This booklet has been designed to explain your operation, hospital stay and recovery. If you need any further information please contact us for advice:
Colorectal Cancer Nurse Specialist, 01908 996 953
Stoma Care Nurse Specialist 01908 996 951
Please leave a message on our answer machine if we are not in the office.